
Liver
is a vital organ, which has regenerative property. Liver functions include
metabolism, digestion, storage, synthesis and release of vitamins, carbohydrates,
proteins and lipids. It also detoxifies and inactivates endogenous and exogenous
substances including toxins and metals.
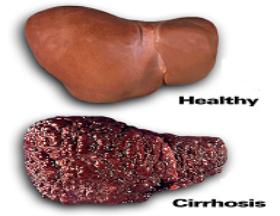
Liver
Cirrhosis and liver circulation
Liver
cirrhosis is one of the diseases of liver, which is caused by different reasons
like alcohol excess, chronic viral hepatitis, drugs and chemicals etc. Cirrhosis
is a condition of severe damage to the liver that impairs its ability to function
normally. It causes formation of scar tissue. This scarring distorts the normal
structure, functions and re-growth of liver cells.
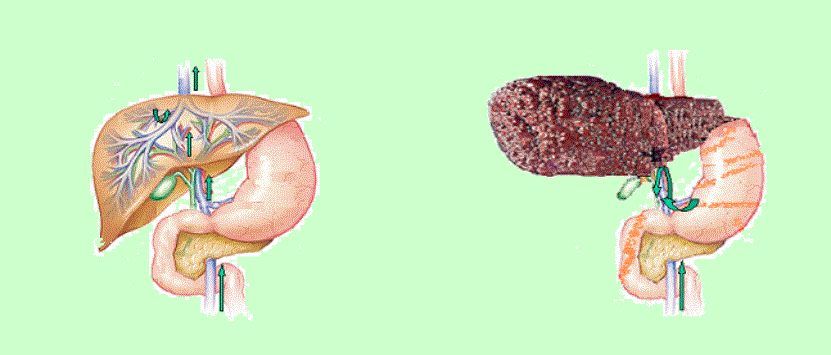
Circulation in
Normal Liver
Hepatic
circulation is a portal system. First blood has to pass through splanchnic
and then hepatic capillary. Blood enter liver through portal vein and
hepatic artery but the out flow is only by hepatic vein. Portal vein
carries blood from the spleen and other digestive organs whereas hepatic
artery carries oxygenated blood from heart. Central vein carries the
detoxified blood from the liver to the heart.
Circulation
in Cirrhotic Liver
In
cirrhotic liver blood vessels inside the liver lobule are partially
blocked due the formation of excess collagen fiber in the liver. Blood
coming from the spleen cannot able to enter liver which increases intrahepatic
resistance to blood flows resulting in hepatic insufficiency and portal
hypertension.
Portal hypertension
Portal
pressure is described mathematically as a function of flow and resistance
across the hepatic vasculature. In cirrhosis, increased intrahepatic
resistance results from both intrahepatic vasoconstriction and surrounding
mechanical factors including collagen deposition and regenerative nodules.
Within the splanchnic and systemic circulation there is increased cardiac
output and hyperdynamic circulation that contributes to increased flow
into the portal circulation thereby perpetuating portal hypertension.
Hepatic Stellate
Cells (HSCs) and Liver Cirrhosis
HSC
Physiology
Hepatic
Stellate Cells (HSCs) are vitamin A storing perisinusoidal pericytes that
undergo phenotypic changes characterized as “myfibroblastic activation”
during liver cirrhosis. Activated HSCs produce fibrosis factors such as collagen,
which leads to the formation of scar tissue in liver and therefore increases
intra hepatic resistance to blood flow. This is how stressed liver ultimately
slips into hepatic insufficiency and portal hypertension.
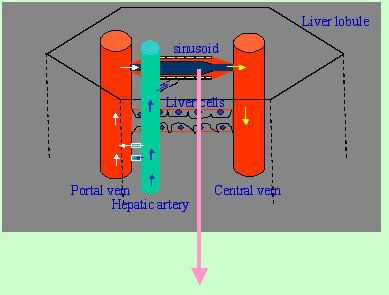 |
The left lobe of
the liver gets blood from the spleen and the right lobe of the liver get
it from the superior mesenteric vein. The portal vein and the hepatic
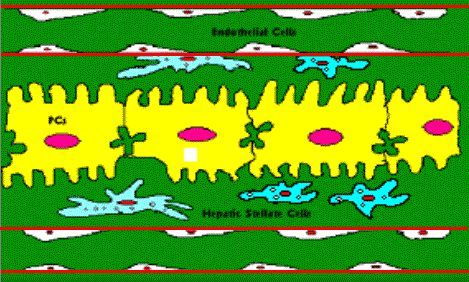
artery have anastomotic connection with the sinusoid. Sinusoid is a smooth-walled
cylindrical tube and is lined by phagocytic cells (Kupffer).
|
 |
Sinusoid consists
of endothelial cell lining having large pores, through which substances
in the plasma move freely into the space of disse. Hepatic stellate cells
exist just beneath the endothelial cell lineage of the blood vessel.
|
HSC Pathology
Hepatic
Stellate cells number increases from normal 3% to 15% during liver cirrhosis.
HSCs and sinusoidal endothelial cells exist in close proximity to each
other in hepatic sinusoid. The hepatic stellate cells (HSC) are now
well established as the key cellular element involved in the development
of hepatic fibrosis.
 |
Hepatic stellate
cell percentage increases from 3% to 15% during cirrhotic condition which
can lead to cross talk between hepatic stellate cells and endothelial
cells in different way than in normal sinusoid. |
During
liver cirrhosis cross talk between activated HSCs and sinusoidal endothelial
cells may lead to remodeling of hepatic sinusoid.
Group’s
objectives
Hepatic
stellate cells and endothelial cells: Do they cross talk?
If
yes in what language do they talk – dissection of pathways.
Modalities
of nitric oxide-use as a therapeutic mean to rectify erroneous cross
talk between HSC and EC?
Possible
Experimental Approaches
1.
Nitric Oxide Donors
Different
nitric oxide donors are used as therapeutic entities for liver cirrhosis.
These are non-specific donors like SNP used for the treatment of liver
cirrhosis (Webb DJ etal. Gut, 2003)
2.
Targeted NO delivery
There are
different liver specific NO donors such as NCX1000 and V-PYRRO-NO which specifically
donate NO to the liver. NCX-1000 is a NO releasing derivative of ursodeoxycholic
acid. Treatment with NCX-1000 resulted in decreased hepatic vasculature resistance;
vasoconstrictor responses without affecting systemic homodynamic and increased
cyclic GMP levels (Stefano Fiorucci etal, PNAS, 2001 and Shah etal. Journal
of Hepatology, 2006).
3.
NOS gene therapy
Delivering
NOS gene using viral vector in cirrhotic rat (Shah etal. AJPGI, 2006)

Our working models
Cell based model of HSC-EC cross talk in liver cirrhosis
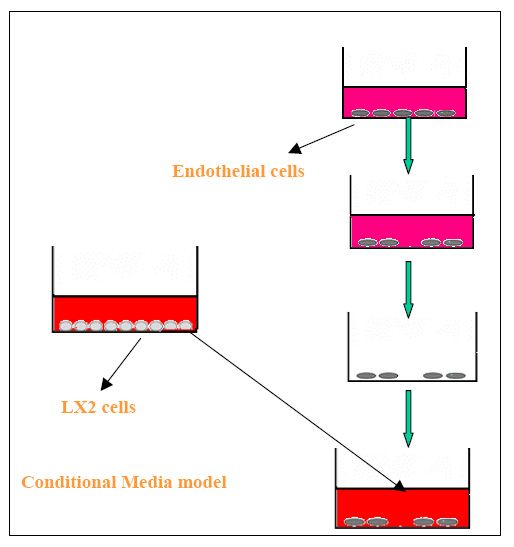
Conditional
media
Here
the hepatic pericytes (here pericyte model is hepatic stellate cells)
grown media is used in order to check the effect of the components released
by pericytes on endothelial cells.
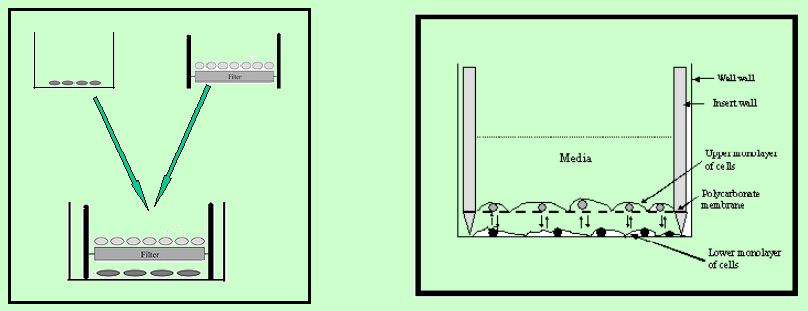
Co-culture
model
This
model mimics the situation of liver sinusoid where hepatic stellate
cells and endothelial cell lineage exist very close to each other and
can able to affect each other’s activity. We are using this model
in order to find out the effect of hepatic stellate cells on endothelial
cells.
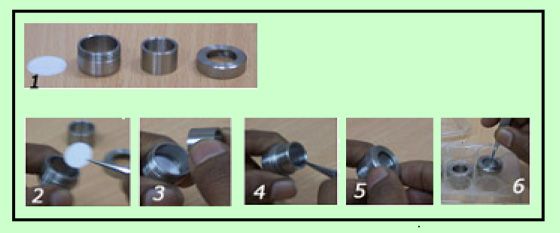
Figure
1
showing the parts of the co-culture chamber (membrane and internal parts.)
Figure 2 Membrane is placed inside the chamber
in order to grow cells upon the membrane. Figure 3
and 4 Membrane supporting part of the co-culture
chamber is placed inside to hold the membrane in place. Figure
5 Upper part of the co-culture chamber is tightened in order to hold
the membrane along with the membrane holder. Figure
6 the whole set up is placed in the 12-well tissue culture plate already
plated with cells. In this set up, it is possible to grow two cell layers
simultaneously as depicted in the upper right cartoon.
Our observations
1)
Activated hepatic stellate cells remodel endothelial monolayer.
2)
Cirrhotic stress alters topography of endothelial cells.
3)
Cirrhotic stress attenuates nitric oxide production by endothelial cells.
4)
Nitric oxide rectifies cirrhosis induced erroneous remodeling
of endothelial monolayer.
Major
groups working in this area:
1. Vijay
H. Shah, Gastroenterology Research Unit, Mayo Clinic, Rochester, MN 55905,
USA
2. Don
C. Rockey, Gastroenterology Division, Duke University Medical Center,
Durham, North Carolina, USA
3. H.
Senoo, Department of Anatomy, Akita University, School of Medicine, Akita,
Japan.
4. Scott
L. Friedman, Icahn Medical Institute, Mount Sinai School of Medicine,
New York
5. Pinzani
M, Dipartimento di Farmacologia Preclinica e Clinica, Italy
Webpage creator:
Syamantak Majumdar
